The CDC updated its COVID-19 isolation policy earlier in March, bringing it in line with recommendations for other respiratory viruses, the flu, and RSV. The key change reduced the recommended isolation time for those with COVID from five days to one after a fever breaks or other symptoms start improving.
The Gazette asked Associate Professor of Epidemiology William Hanage, who is also associate director of the Harvard T.H. Chan School of Public Health’sCenter for Communicable Disease Dynamics, for his take. Hanage pointed out that, though COVID infection, care, and treatment has become more routine recently, many people remain vulnerable, as evidenced by national weekly deaths figures that this winter ranged from 500 to 2,000. This interview was edited for clarity and length.
The CDC’s action seems to be a fairly significant shift. Do you agree with what they’re doing?
It is a significant shift in some ways, but I also think that it’s just the guidance catching up with what’s been out there for a while.
“You should not think that there is no potential for you to transmit after the fever is broken, and if you’d like to be more confident, you can do a rapid test. If you want to be more sure, you can use a mask.”
William Hanage
Nothing spectacular has changed, but over the last year there have been fewer and fewer people even taking a test if they feel that they might have COVID. And of those who do, some might isolate but some of them won’t. And there are people who won’t even take the test because they’re afraid that they’d have to isolate.
The role of CDC is to give people advice that they can actually use. That’s what I think this is.
Having said that, it does not mean that the virus is no longer a threat, in particular to people who are vulnerable. If you look at the number of hospitalizations and look at the number of deaths, there’s been a steady drumbeat over the course of this winter of levels lower than we’ve had in the past but still really pretty darn high in comparison with the amount of respiratory infection we usually see.
And, while flu and RSV are very spiky, COVID has been there more or less continuously. That partially reflects the fact that we continue to have a lot of transmission in our communities and that there continue to be a lot of people out there who could fall seriously ill if they’re unfortunate enough to get it. That’s where we need to focus things and make sure they get boosters.
As we look beyond the top line, the CDC didn’t change recommendations about vulnerable people and people in healthcare institutions.
That’s important to remember because you still really don’t want to introduce this virus — or any respiratory infection — to a nursing home or a healthcare setting. We should be working to come up with ways to clearly communicate that and help people, when they become infected themselves, to avoid infecting others.
That’s a lot easier if you have things like adequate sick pay. If somebody who is working two jobs to put food upon the table falls ill and doesn’t have sick pay, they’re not going to isolate, they will go to work because they have to. They’re also the folks who might not be able to get access to boosters, might not be able to get access to tests. It’s the same channels of inequities that make up the American healthcare system.
I’ve heard people say the virus isn’t that bad anymore, but what has happened is we’ve gained immunity. If this virus today spreads amidst a naive population like we had in 2020, what would be the outcome?
It would be utterly ghastly. It’s a little bit difficult to know exactly how intrinsically transmissible it is, but it’s certainly more transmissible than what we had in 2020.
And it’s no less virulent. We’ve got evidence of that from what happened in Hong Kong, when BA.2 finally went through there. That was really grim — and they had vaccines.
Yet for a period of about a month there were scenes much like those in New York at the start of it all. That reflects how incredibly transmissible this virus is.
It also reflects the fact that it’s never been a big deal for most people but if you infect huge numbers, it will be a big deal for enough of them. That combination means that we are fortunate because we have vaccines; we are fortunate because there is now large amounts of convalescent immunity that came, for many of us, from infections that happened after being vaccinated and getting that protection.
We’re glad about that, but we — meaning the medical community — would still look at this and think, “Wow, that’s a lot of respiratory disease.” I’m delighted that that’s something that I think about but most folks don’t need to, but it’s still the case that we’re not at a point yet where it has returned to anything like what we had before.
And that may well never happen because we have just added another respiratory virus and that has consequences.
CDC numbers show cases way down, but isn’t that a great underestimate because nobody’s testing anymore, and a lot of cases are asymptomatic?
If you look at things that are somewhat unbiased, like wastewater monitoring, there’s plainly still a lot of infection and transmission happening in the U.S. We don’t pick up on most of it because most people don’t test and don’t get counted. But we do still see hospitalizations and deaths. Those remain high by pre-2020 standards — though low by everything we’ve seen since then.
The risk is concentrated among those in whom it’s been concentrated all along: older folks, people with comorbidities, and the like. But your average person in the street is not going to be thinking about COVID all the time and frankly, I don’t think they need to.
But I would love it if more folks in that category were conscious of the potential to make somebody sick, someone not as lucky as them. And there’s loads of things you can do to make that less likely.
A day after your fever breaks, I imagine you’re more infectious than you would be after five. Does that highlight the importance of some of the things that have been de-emphasized, like masking and fresh air?
You should not think that there is no potential for you to transmit after the fever is broken, and if you’d like to be more confident, you can do a rapid test. If you want to be more sure, you can use a mask.
But a lot of the symptoms that people are getting are in part connected to the immunity they have. So, when your immune system kicks off, it creates a bunch of symptoms — the things that make us feel cruddy.
And there is a connection between replicating virus and symptoms. What that means is that there is less presymptomatic transmission than earlier in the pandemic, and there’s also less transmission after things have resolved. That means that you should try to avoid exposing people when you have symptoms. That’s true for COVID and for any of the other viruses as well.
Is this likely the final step in normalizing COVID? Does the CDC still need to do anything else on this front?
I hope that they’re never going to say that nobody needs to pay attention to COVID, to whether they’re exposing people in nursing homes. But it is certainly a point in the pandemic that represents the way that public health has normalized it.
We will still be encouraging people to get boosters. We will still be warning people ahead of respiratory virus season to keep an eye out and not infect their vulnerable neighbors. And we will still be working to find ways to minimize the impact of the virus. That’s all stuff that’s going to be going on in the background. And we’ll keep doing our best to reduce preventable suffering and death — there’s still a lot we can do.
Including surveillance, keeping an eye out for new variants?
Yes, that includes keeping an eye out for when things are going to be getting better, or for when things could be getting bad. We’re not going to go back to where we were, but despite the virus continuing to evolve, despite the virus continuing to be with us, despite there continuing to be significant amounts of sickness and death, it’s nowhere near the pandemic levels — those huge spikes.
We should take a deep breath and feel good about that, while at the same time recognizing that just because only one of your houses is on fire, it’s not a reason not to try and put it out.
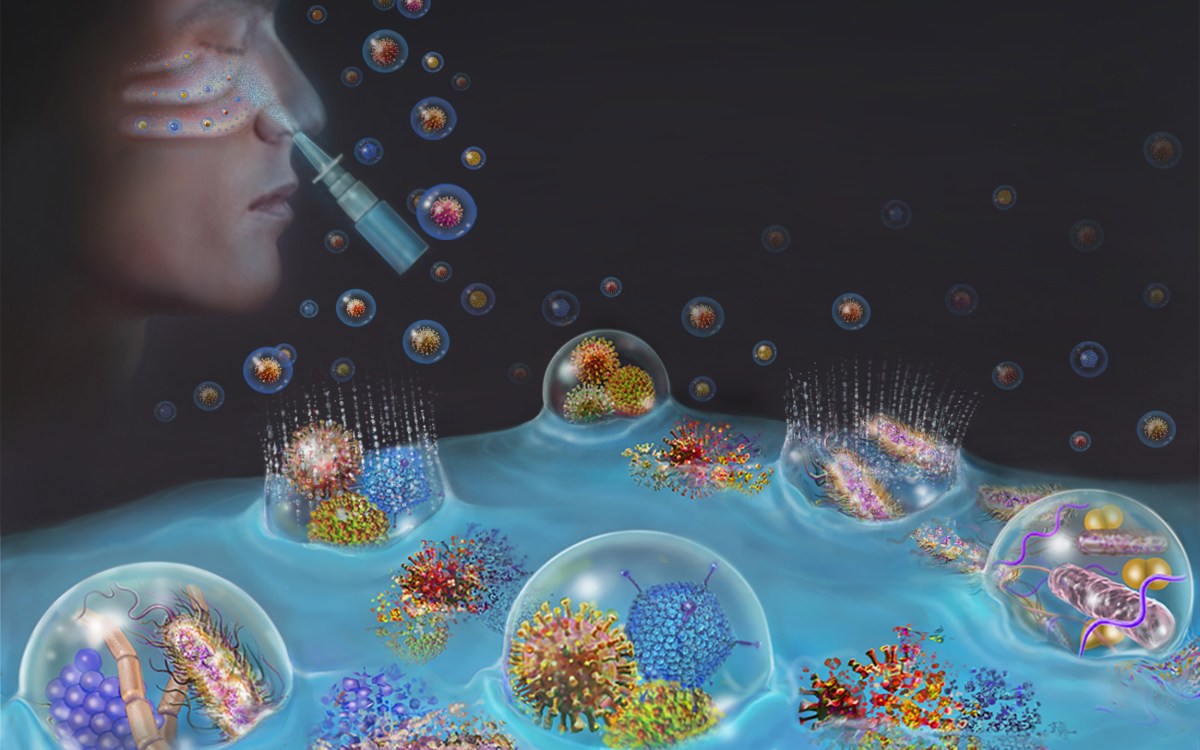
In preclinical studies, spray offered nearly 100% protection from respiratory infections by COVID-19, influenza, viruses, and pneumonia-causing bacteria